Black people who die from COVID are about 10 years younger than whites who die from the virus. Vaccinating strictly by age leaves some Black people out, experts say
Written by Wendi C. Thomas and Hannah Grabenstein
Published on 12th February 2021

Rosalyn Campbell and her husband, Calvin, are waiting for what may be the most in-demand item on the planet: the COVID-19 vaccine. They both caught the virus in November; Calvin Campbell tested positive just days after he’d been released from the hospital following open heart surgery.
After a weeklong stint in the hospital, he returned to his job as a buildings and grounds engineer, where he’s on light duty. But Rosalyn Campbell, who also has a heart condition, remains anxious.
“I’ve got to have it. … I want this behind me,” said Campbell, who retired from FedEx in 2013.
But it may be March before the couple, who are both Black and 65, are eligible to get the vaccine, based on the state’s age-based vaccination plan. Tennessee, like most states, gave first priority to those 75 and over, following the advice of the Centers for Disease Control and Prevention. As the virus’s death toll climbs to more than 465,000 nationwide, policymakers around the country are struggling to inject equity into vaccination policies.
Prioritizing by age might seem like an obvious choice, given the disproportionate impact of the disease on the elderly. Setting the initial threshold at 75, however, ignores the fact that a smaller share of Black people reach that age than white people. It also fails to account for research, released by the nonprofit Brookings Institution in June, showing that Black people who die of COVID-19 are, on average, about 10 years younger than white victims of the disease. (Data for Shelby County, Tennessee, where Memphis is located, bears this out as well.)
“If you [allocate the vaccine] strictly by age, you’re going to vaccinate white people who have lower risks before you vaccinate Black people with higher risks,” said Sarah Reber, co-author of the Brookings research and associate public policy professor at the UCLA Luskin School of Public Affairs.
“If you’re trying to avert deaths, you would want to vaccinate Blacks who are about 10 years younger than whites.”
The pandemic is expected to lower life expectancies nationwide, which will only exacerbate the Black-white life-expectancy gap. Before the pandemic, Black residents of Shelby County, on average, were expected to live to be 73 years and four months old, compared to 78 years and one month for white residents. What that means is that while 54% of the county’s residents are Black, Black people account for only 39% of residents 75 and up.
In Shelby County, the poverty rate is 25% higher than the statewide rate, and the residents who live below the poverty line are concentrated inside Memphis city limits.
Shelby County Residents 75 And Older Are Disproportionately White
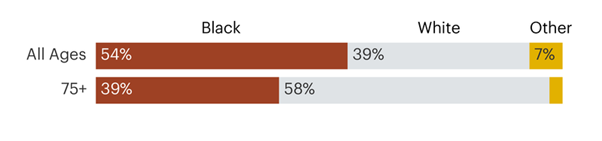
Credit: Source: American Community Survey, 2019
Data from around the country — and from cities such as Washington, D.C., and Chicago — reveal vast disparities between where COVID-19 is hitting hardest and where shots are making it into arms. The latest national government data shows that when the race of the person getting the vaccine is known, Black residents are underrepresented; just over 5% of vaccine recipients were Black, compared to just over 60% who were white. By contrast, about 12% of the U.S. population is Black and 60% is white.
The population of Shelby County is 54% Black and 35% white. As of Feb. 6, 22% of Shelby County vaccine recipients are Black, compared to 43% who are white. (Around 16% are categorized as “Other/Multiracial/Asian,” while the remaining 18% or so are unknown).
Experts attribute the vaccination disparity to a number of factors, including poor internet access, lack of transportation and distrust of the medical system caused by racist practices such as the federal government’s Tuskegee syphilis study. The distrust becomes visible in a recent Kaiser Family Foundation survey in which a much higher share of Black people than white say they prefer to wait and see how the vaccine works before receiving it. (An equal share of white and Black respondents — 14% — say they definitely won’t get vaccinated.)
But these disparities aside, strict age cutoffs also play a role. Calculating the impact of those cutoffs is difficult because the age criteria are shifting downward as the rollout plan advances. Last week, the Shelby County Health Department announced that people over 70 are now eligible to be vaccinated. But that is unlikely to fully address the inequity built into the age-based system.
According to the state’s health disparities dashboard, Black residents of Shelby County have higher rates of infections, hospitalizations and mortality than white residents. Among residents between 65 and 74 whose race is known, Black people are notably overrepresented in COVID-19 fatalities, according to the SCHD, making up 67% of deaths in that age range, compared to 28% for white residents, as of Jan. 31.
COVID-19 Disproportionately Kills Black Residents Ages 65-74 Compared To White Residents
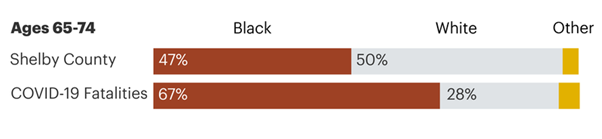
Note: The health department did not have race information for 10 of the 315 people in this age bracket who have died of COVID-19. Credit: Source: American Community Survey, 2019, Shelby County Health Department
Even before the vaccine rollout, some experts warned about the racial implications of prioritizing by age. Before the CDC issued its recommendations, a Chicago health disparities researcher and bioethicist raised her concerns about a “one-size-fits-all” age threshold during the public comments at a December CDC committee meeting.
“The burden of COVID mortality that we’re seeing in minority communities has shifted to much younger populations than what we are seeing in the non-minority populations,” said Dr. Monica Peek, an associate professor and physician at the University of Chicago.
The Tricky Balance of Efficiency and Equity
From the start of the pandemic, it has been clear how much harder communities of color have been hit. Late last month, two senators and a congresswoman from Massachusetts, all Democrats, sent a letter to the U.S. Department of Health and Human Services. “It is critical that the federal government’s vaccine deployment campaign does not fail the communities that have been forced to shoulder the greatest burden,” it read.
But reddressing that disparity in a vaccination rollout plan proved difficult. Reporting by MLK50 and ProPublica opens a window on those debates. The Advisory Committee on Immunization Practices, a CDC group of vaccinologists and medical and public health experts, was responsible for developing a national framework for vaccine approval and distribution. An ACIP work group decided in November to ground their work in four ethical principles: Maximize benefits and minimize harms, promote justice, mitigate health inequities, and promote transparency.
Meeting minutes reveal that ACIP examined data showing Black and Hispanic/Latino people are disproportionately hospitalized for and die from COVID-19. They’re also overrepresented in essential occupations, where opportunities for exposure are more common, and underrepresented in older age groups.
Questions about how to handle race and ethnicity surfaced at the group’s June meeting. “How should racial and ethnic groups at high risk for severe COVID-19 be prioritized? Should race and ethnicity be a criterion for vaccine prioritization?” read the June meeting summary.
Four months later, ACIP answered its own questions. “It is critical for ACIP to address equity and disproportionate impact on disadvantaged populations,” reads the October meeting summary. But, the notes continue, “approaching this from a race/ethnicity standpoint is probably not the best approach.”
Prioritizing one group over another inevitably pushes others to the back of the line, experts say, and it’s not clear whether governments could legally specify different age cutoffs by race, or whether it would be feasible politically or possible logistically.
“In general, our country is very reluctant to encode racial categories into law,” said Elizabeth Wrigley-Field, assistant professor of sociology at the University of Minnesota. Wrigley-Field, who is not on the ACIP committee, recently published research on racial inequality and life expectancy that suggests racism may be as deadly as the pandemic.
In some communities that have tried more race-specific solutions for vaccine distribution, the blowback has been swift. After early data showed residents in affluent and predominantly white neighborhoods were the primary vaccine recipients, the Dallas, Texas, County Commission decided in mid-January to target the most vulnerable ZIP codes. The very next day, Texas health officials announced that the state would shrink Dallas County’s vaccine allocation unless it abandoned the plan, which the county did.
Tennessee’s vaccination plan states that “equity remains a crosscutting consideration,” and sets aside 5% of its weekly vaccine allocation for counties, including Shelby, that rank high on the CDC’s social vulnerability index, which includes race as one of 15 factors.
“This allows those counties to vaccinate more people more quickly and move ahead in the phases,” said Tennessee Department of Health spokesperson Bill Christian in an email. He didn’t answer questions about how many doses Shelby County receives or if the doses are distributed based on population; to date, those numbers have not been made public.
Although ACIP and the CDC recommended the social vulnerability index as a proxy for race, that was a mistake, said Dr. Uché Blackstock, an emergency physician and CEO and founder of Advancing Health Equity, a national group that works with health care institutions to address health inequities. “That was an opportunity for the federal advisory committee to really make a statement about how racism has essentially created environments and limited opportunities,” she said. “Racism so explicitly harms Black people, but then in terms of addressing that and mitigating the impact of racism, we cannot use race explicitly.”
The Shelby County Divide
While COVID-19 is expected to lower the country’s life expectancy by more than a year, for Black residents, it will drop by more than five years, wiping away reductions in the Black-white gap made over the last 15 years, according to research from the University of Southern California and Princeton.
On a census tract level, the life expectancy disparities in Shelby County become even more stark. Even pre-COVID-19, the gap between a virtually all-white suburban census tract and a virtually all-Black one in Memphis stood at more than 19 years.
The county’s census tract with the highest life expectancy, 84.6 years, is in the suburban town of Collierville, in a neighborhood where some street names — Scarlett’s Way, Rhett’s Way and Taraview — are inspired by “Gone With The Wind.” Here the population is 96% white, the poverty rate is less than 1%, and the median household income of nearly $108,000 is twice that of the county.
More than 20 miles west is the neighborhood with the lowest life expectancy — 65.3 years. It sits in South Memphis, where a boulevard bears the name of a wealthy developer. The census tract is 96% Black, with a 42% poverty rate and a median household income of less than $20,000, less than half of the county’s.
Campbell and her husband live about 6 miles away, in a predominantly Black part of Memphis called Whitehaven. In her neighborhood, the life expectancy is 74.5 years, just shy of the 75 and older age bracket that was first to get the vaccine.
Both Campbell and her oldest sister, retired educator Linda Williams, live in almost all-Black census tracts where the poverty rate is higher than the county’s and household income is lower. The life expectancy in Williams’ neighborhood is even shorter, at 71.7 years. Williams, 69, recalls fondly her pre-pandemic life. In the before times, she kept busy with water Zumba and water aerobics. Now, she exercises on a stationary bike that sits near a window so she can look outside. “Can’t go to church, can’t go anywhere,” she said. Late last year, she lost a friend of 30 years to the virus, and she’s eager for the vaccine. “You see the numbers on the screen, but … it hits you different when you actually know the person,” she said.
Struggling With Equitable Distribution and Access
Of course, being eligible to receive the vaccine isn’t the same as being able to access it. And the vaccination rollout in Shelby County, as in other communities, has been troubled in ways that worsen racial inequities.
As of Feb. 1, 24 states, including Tennessee, were publicly reporting COVID-19 vaccination figures by race and ethnicity, according to the Kaiser Family Foundation. As of Feb. 10, less than 7% of the state’s vaccine recipients were Black, compared to about 17% of the state’s population.
As of Feb. 6, Shelby County’s vaccination rates have been highest along the Poplar Avenue corridor, a predominantly white swath of town that starts at the Mississippi River and runs southeast toward the county’s more affluent suburbs. Rates are far lower in the largely Black and less-affluent ZIP codes north and south of the Poplar corridor.
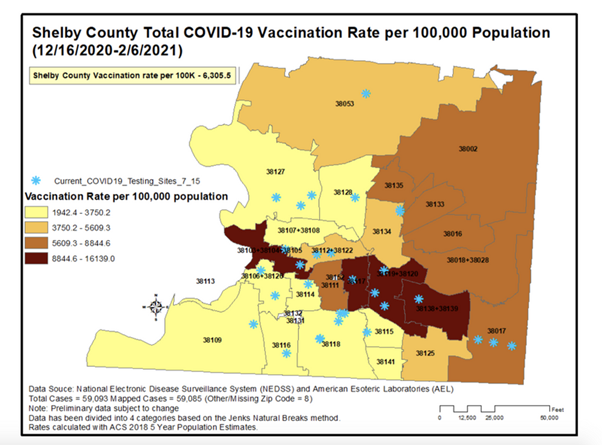
Credit: Source: Shelby County Health Department